These resources are designed to support you in identifying which patients may benefit from genetic testing, navigating the process, and helping families interpret results.
Help guide your patients’ genetic testing journey.

Expert Organizations
Expert groups provide guidelines and recommendations around genetic testing, helping you know when testing might be helpful for your patients.
FAQs
We’ve developed the following FAQs to support clinical decision-making at every stage of the genetic testing process.
Indications for genetic testing according to the American College of Medical Genetics and Genomics (ACMG) and/or American Academy of Pediatrics (AAP):
- Developmental delay
- Developmental regression
- Intellectual disability
- Autism
- Growth differences, such as poor growth, or overgrowth
- Birth defects
- Congenital hearing loss
- Cerebral palsy
There are many reasons that genetic testing should be considered. For pediatric patients having neurodevelopmental features, the ACMG has genetic testing practice guidelines, here.
While ACMG does not have guidelines for patients with epilepsy alone, professional recommendations curated by the National Society of Genetic Counselors (NSGC) for unexplained epilepsy were published in 2022.
It is important to note to patients and their families that a genetic diagnosis explains the genetic etiology of a patient’s medical features but does not establish clinical diagnoses such as autism, which relies on a set of behavioral characteristics to have a diagnosis
There are many potential benefits of receiving a genetic diagnosis, including (Ledbetter et al 2025):
- Allowing more accurate prognostication of long-term outcomes
- Facilitating timely identification and treatment of co-occurring medical conditions
- Informing genetic counseling about the chance of recurrence in future pregnancies
- Refining selection of treatment options for those who need them
- Identifying support and advocacy resources
- Ending the diagnostic odyssey for families
References
Ledbetter D, Finucane B, MorenoDeLuca D, Myers S. Mainstreaming diagnostic genetic testing and precision medicine for autism spectrum disorder. Psychiatr Clin N Am (2025)
DOI: 10.1016/j.psc.2025.01.010
There are several different types of diagnostic genetic tests; this does not include genetic screening tests such as what is used in prenatal screening or direct-toconsumer testing.
Genetic testing used in a pediatric clinic includes: karyotype, chromosomal microarray, gene panel, exome sequencing and genome sequencing. The following table includes some details about these different tests.
| Type | Description | Limitation | General uses | Recommendations & guidelines |
|---|---|---|---|---|
| Karyotyping or chromosome analysis | Used to investigate chromosome structure, large genetic variations. | Not able to detect genetic variations smaller than 5–10 MB, meaning it can only detect larger structural differences. | For chromosomal abnormalities such as Down syndrome, extra or missing pieces of genetic material, or whole chromosomes, including translocations. | Can be considered for prenatal investigations, family history of chromosomal disorders, previous child with a chromosomal abnormality, if one or both parents are carriers of balanced chromosomal rearrangements or in cases of recurrent miscarriages1,2 |
| Chromosomal Microarray Analysis (CMA) | Used to detect extra or missing genetic information, can pick up on smaller genetic variants than karyotype. | Cannot consistently detect copy number variations (CNVs) smaller than 100–200 kilobases (KB), and single nucleotide differences or balanced chromosomal rearrangements. | Used for identifying causes of autism, developmental delay, or intellectual disability. | Can be considered for patients with single developmental diagnoses (autism, or intellectual disability etc).2,3,4 |
| Gene panel | A list of genes sequenced in high detail relating to a particular genetic condition. Will be different from lab to lab. | Variants of uncertain significance are common, and might not detect large deletions or duplications, and cannot detect balanced chromosomal rearrangements. | Used for specific clinical diagnoses, such as autism, epilepsy, or intellectual disability. | There are no current professional recommendations for ordering a gene panel for a genetic condition; this often is a consideration if previous genetic testing was negative, if covered by insurance and if the person’s clinical presentation fits the gene panel investigation. |
| Exome sequencing | Sequencing of a person's exons, the genes that code for proteins (coding region) of the genome. | Variants of uncertain significance are common and cannot detect balanced chromosomal rearrangements. | Used when it is strongly suspected a person has a genetic condition and other testing was negative, or in certain neurodevelopmental and/or congenital malformations. | Can be considered as an appropriate test for someone with congenital anomalies with onset prior to age 1 year, seizures or other neurologic abnormalities, developmental delay or intellectual disability with onset prior to age 18 years.5,6,7 |
| Genome sequencing | A sequencing of a person's entire genome, coding and non-coding. | Variants of uncertain significance are common, in addition to a lot of data that may be difficult to interpret. | Sometimes used when it is strongly suspected a person has a genetic condition and other testing was negative, or in certain neurodevelopmental and/or congenital malformations. | Can be considered as an appropriate test for someone with congenital anomalies with onset prior to age 1 year or developmental delay or intellectual disability with onset prior to age 18 years.5,6,7 |
- de Assis V, Giugni CS, Ros ST. Evaluation of Recurrent Pregnancy Loss. Obstet Gynecol. 2024;143(5):645-659. doi:10.1097/AOG.0000000000005498
- Silva M, de Leeuw N, Mann K, et al. European guidelines for constitutional cytogenomic analysis. Eur J Hum Genet. 2019;27(1):1-16. doi:10.1038/s41431-018-0244-x
- Schaefer, G. B., Mendelsohn, N. J. & Professional Practice and Guidelines Committee. Clinical genetics evaluation in identifying the etiology of autism spectrum disorders: 2013 guideline revisions. Genet. Med. 15, 399–407 (2013).
- Shao L, Akkari Y, Cooley LD, et al. Chromosomal microarray analysis, including constitutional and neoplastic disease applications, 2021 revision: a technical standard of the American College of Medical Genetics and Genomics (ACMG). Genet Med. 2021;23(10):1818-1829. doi:10.1038/s41436-021-01214-w
- Manickam, K. et al. Exome and genome sequencing for pediatric patients with congenital anomalies or intellectual disability: an evidence-based clinical guideline of the American College of Medical Genetics and Genomics (ACMG). Genet. Med. 23, 2029–2037 (2021).
- Malinowski J, Miller DT, Demmer L, et al. Systematic evidence-based review: outcomes from exome and genome sequencing for pediatric patients with congenital anomalies or intellectual disability. Genet Med. 2020;22(6):986-1004. doi:10.1038/s41436-020-0771-z
- Rodan LH, Stoler J, Chen E, Geleske T; Council on Genetics . Genetic Evaluation of the Child With Intellectual Disability or Global Developmental Delay: Clinical Report. Pediatrics. 2025;156(1):e2025072219. doi:10.1542/peds.2025-072219
Most outpatient genetic testing requires prior authorization from the insurance to be considered for coverage. Genetic testing labs may assist with this process and obtain prior authorization on behalf of the ordering provider or perform a “benefits investigation” that will provide an estimated out-of-pocket expense based on the individual’s specific insurance policy. However, these are estimates, so patients should never be told that insurance will or will not cover testing without speaking with the lab or insurance company directly.
Insurance companies have different coverage policies and criteria for genetic testing. Therefore, careful review of a specific payor’s policy can be helpful in determining if genetic testing may be covered. In addition, these policies may change over time as new publications supporting the utility of genetic testing are published, so it is important to remain up-to-date with different insurance policies and/or contact the genetic testing lab for further guidance.
Medicaid policies for genetic testing coverage vary by state. Information on different states' Medicaid coverage for genetic testing can be found here: genetic testing. Please note that Medicaid coverage policies may mirror commercial insurance policy requirements for justification of medical necessity.
In addition, genetic testing labs are often available to help navigate the nuances of genetic testing and insurance coverage for their patients, so test-specific or insurance-specific questions can be directed to the lab providing the test.
In general, payors want to understand how the genetic testing and diagnosis will directly impact the medical management of the individual. Therefore, documenting in your clinic note or recommendations how the testing will directly impact medical management (e.g., recommending screening or surveillance based on the specific medical management and natural history of the condition, reducing unnecessary tests or imaging orders, etc.) can be helpful.
In the event of a denial, some insurance carriers may allow providers to appeal or schedule a peer-to-peer review, where the provider will have the opportunity to discuss the medical necessity of the genetic testing with a medical provider from the insurance company.
When ordering genetic testing, you should ensure that the genetic testing company can return clinical-grade testing results. This is typically achieved by using a laboratory that is CLIA and/or CAP certified. Many laboratories worldwide hold these accreditations.
CLIA (Clinical Laboratory Improvement Amendments) refers to genetic tests performed in laboratories certified under the CLIA program, which ensures that they meet federal standards for the quality, accuracy, and reliability of testing.
CAP (College of American Pathologists) offers an additional, voluntary accreditation for clinical testing laboratories. Its Laboratory Accreditation Program provides a rigorous process through which laboratories can demonstrate their commitment to quality and patient safety.
Globally, genetic counseling is becoming more widely available. Table 3 in this recent publication by Ormond et al., 2024, reviews the various genetics and genetic counseling governing bodies globally.1 If looking for genetic counseling in a particular country, please review Tables 2 and 3 in that publication, and Table 3 included below. *
References
Ormond KE, Abad PJ, MacLeod R, Nishigaki M, Wessels TM. The global status of genetic counselors in 2023: What has changed in the past 5 years? Genet Med Open. 2024;2(Suppl 2):101887. Published 2024 Aug 8. DOI: 10.1016/j.gimo.2024.101887
| Country/Region | Organization | |
|---|---|---|
| International/Regional organizations | ||
| Asia | PSGCA | |
| Europe | ESHG | |
| EBMG | ||
| Latin America | SPLAGEN | |
| Various countries | Transnational Alliance of Genetic Counseling | |
| Various countries | ASGC | |
| Country organizations | ||
| North America | ||
| Canada | CAGC | |
| Association des conseilleres et conseillers en genetique de Quebec - Quebec Association of Genetic Counsellors | ||
| OAGC-ACGO | ||
| United States of America | NSGC | |
| ABGC | ||
| ACGC | ||
| AGCPD | ||
| Central and South America | ||
| Mexico | AMGH | |
| CMG | ||
| Europe | ||
| Austria | ÖGH | |
| Belgium | BeSHG | |
| Denmark | DSMG | |
| France | AFCG | |
| Germany | GFH | |
| Italy | Societa Italiana di Genetica Umana | |
| Netherlands | VKGN | |
| Malta | GGCAM | |
| Norway | NSHG | |
| Norwegian Interest Association for Genetic Conseling | ||
| Portugal | APPAcGen | |
| SPGH | ||
| Romania | Romanian Association for Genetic Counseling | |
| Spain | SEAGen | |
| Sweden | SFGV | |
| SFMG | ||
| Switzerland | Swiss Association of Genetic Counselors | |
| United Kingdom | AGNC | |
| Asia | ||
| China | CBGC | |
| Hong Kong SAR | HKSGC | |
| India | BGCI | |
| Indonesia | InaSHG | |
| ISGC | ||
| Japan | JACGC | |
| JSGC | ||
| Malaysia | GCSM | |
| Philippines | PSGC | |
| Singapore | GCSS | |
| South Korea | KSMG | |
| Taiwan | Taiwan Association of Genetic Counseling | |
| Thailand | MGGA | |
| Middle East | ||
| Israel | Israeli Association of Genetic Counselors | |
| Oman | Oman Society of Medical Genetics | |
| Saudi Arabia | Saudi Network of Genetic Counselors | |
| SSMG | ||
| Turkiye | TGD | |
| Africa | ||
| South Africa | GC-SA | |
| Oceania | ||
| Australia and New Zealand | HGSA | |
| ASGC | ||
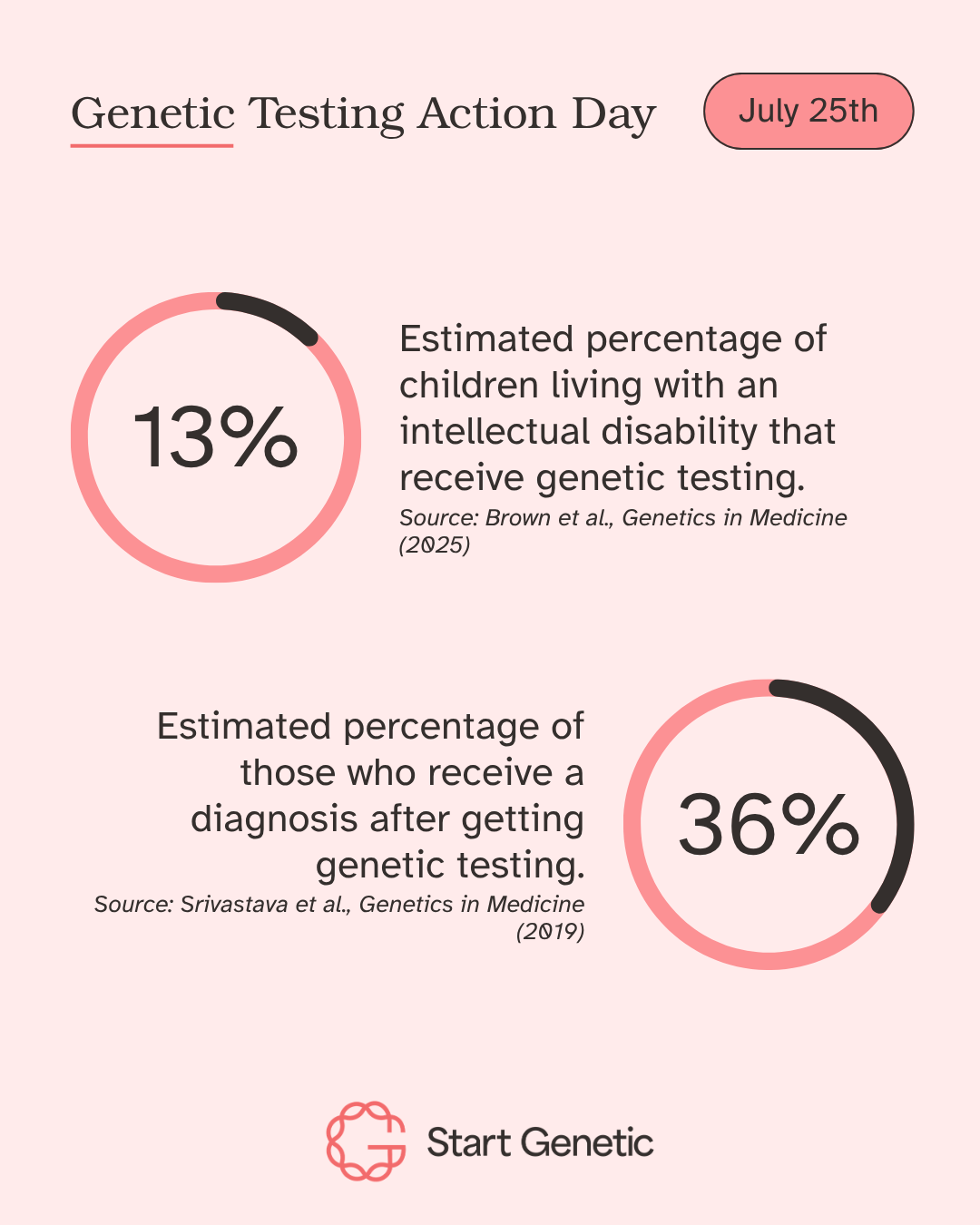
If no genetic change is identified, a referral to a genetics provider may still be indicated. Currently, genetic testing identifies a cause for an individual’s medical or developmental concerns approximately 30-40% of the time.
Therefore, most of the time, genetic testing may come back as “normal”, “negative”, or “non-diagnostic”.
This does not mean that the individual does not have a genetic etiology for their symptoms, it may just mean that we have not discovered the genetic cause yet.
Therefore, evaluation by a genetics provider and reanalysis of previous non-diagnostic genetic testing over subsequent years may be indicated.
The Genetic Information Nondiscrimination Act (GINA) protects individuals against discrimination based on their genetic information in health coverage and in employment. However, this law does not apply to health insurance if a company has less than 15 employees, life insurance, disability, or long-term care insurance. For additional information regarding GINA, please see here.

Resources for Patients
Looking for materials to share with families? Direct them to our Patients and Families page for plain language guides on genetic testing, pathways to care, and finding community support.

Take Action
Your role in this movement matters. Every referral, conversation, or test ordered is a step toward answers for a family that needs them. Visit our Take Action page to learn more about how you can advocate for genetic testing – helping to expand access in your practice and beyond.